CBBLE UDHC Similar cases
I have been given this case to solve in an attempt to understand the topic of "Patient Clinical Data Analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and diagnosis with a treatment plan.
This is an online E log book to discuss our patient’s de-identified health data shared after taking his guardian’s signed informed consent.
A 75 year old woman came with chief complaints of
- Involuntary movement of hands and head bobbing since 7AM 22/2/22
- Burning micturition since 1 week
Patient was apparently asymptomatic 10 days back and then developed fever which was insidious in onset, continuous and subsided with medication.
- Involuntary movement of hands and bobbing of head at frequent intervals seen.
- Frequent episodes of burning micturition which subsided on medication present. This time inspite of usage of same medication she isn’t feeling better.
- There was sudden onset of shivering since morning and burning micturition since one week associated with chills,Right flank pain present, increased frequency of micturition at night.
- Patient is conscious but only responding to some questions, and giving only monosyllable responses.
- She was active till today morning and performed her routine activities and maintained hygiene. She couldn’t cook for herself since 5-6 months as she couldn’t light the stove.
- History of fall 13 years back, she injured her knee. History of massage of knee after injury,non healing of injury and discharge from the wound present. Skin grafting done sit to non healing of wound.
On check up for fall, she was diagnosed with Diabetes mellitus and Hypertension and is on regular medication for it (Tab. METFORMIN 500mg and Tab. MET XL)
- History of fall 10years back and fractured her wrist at that time.
- Using medication (Tab. ROSUVASTATIN,CLOPIDOGREL&ASPIRIN combination) for heart problem. On enquiry about the heart problem, the patient’s attender said that the patient complained of weakness so was taken to a doctor who said, there is narrowing of vessels and put her on the above medication.
No complaints of chest pain or breathlessness.
Past history:
Was diagnosed with Hypertension and Diabetes mellitus 13 years back and is on regular medication for it.
Drug history:
- Metformin 500mg
- Cefixime and OFLOXACIN
- Met XL
- NODOSIS
- Paracetamol,Aceclofenac and Serratiopeptidase
- ROSUVASTATIN,CLOPIDOGREL&ASPIRIN
Personal history:
Diet: mixed
Appetite: decreased
Sleep: disturbed
Bowel and bladder movement: burning micturition +, bowel movements normal
Addictions: none
General examination:
Temperature: 97.4°C
PR: 88bpm
BP: 130/70
SpO2: 98%
GRBS: 155mg/dl



CNS Examination:
Patient is conscious, oriented to time, person
Speech - normal
Reflexes -
B. T. S. K. A. P
Rt. + + +. +. +. +
Lt. + + +. +. +. +
Rt. Lt
Tone
UL N. N
LL. N. N
Power rt. Lt
UL. -4/5. -4/5
LL. -4/5. -4/5
Rombergs positive
Proprioception- lost
Cerebellar signs-
Tandem walking - impaired
No nystagmus
UL and LL coordination impaired
Gait:
Investigations:
Hemogram:
Hb: 7.6
TLC: 13,600
N: 90
L: 05
Imp: Normocytic hypochromic anemia with neutrophil leukocytosis
USG ABDOMEN:
Imp: Bilateral RPD changes seen in kidneys.
Ophthalmology referral:
I/V/O raised intracranial pressure.
Imp: optic disc not visualised due to dense lenticular opacities
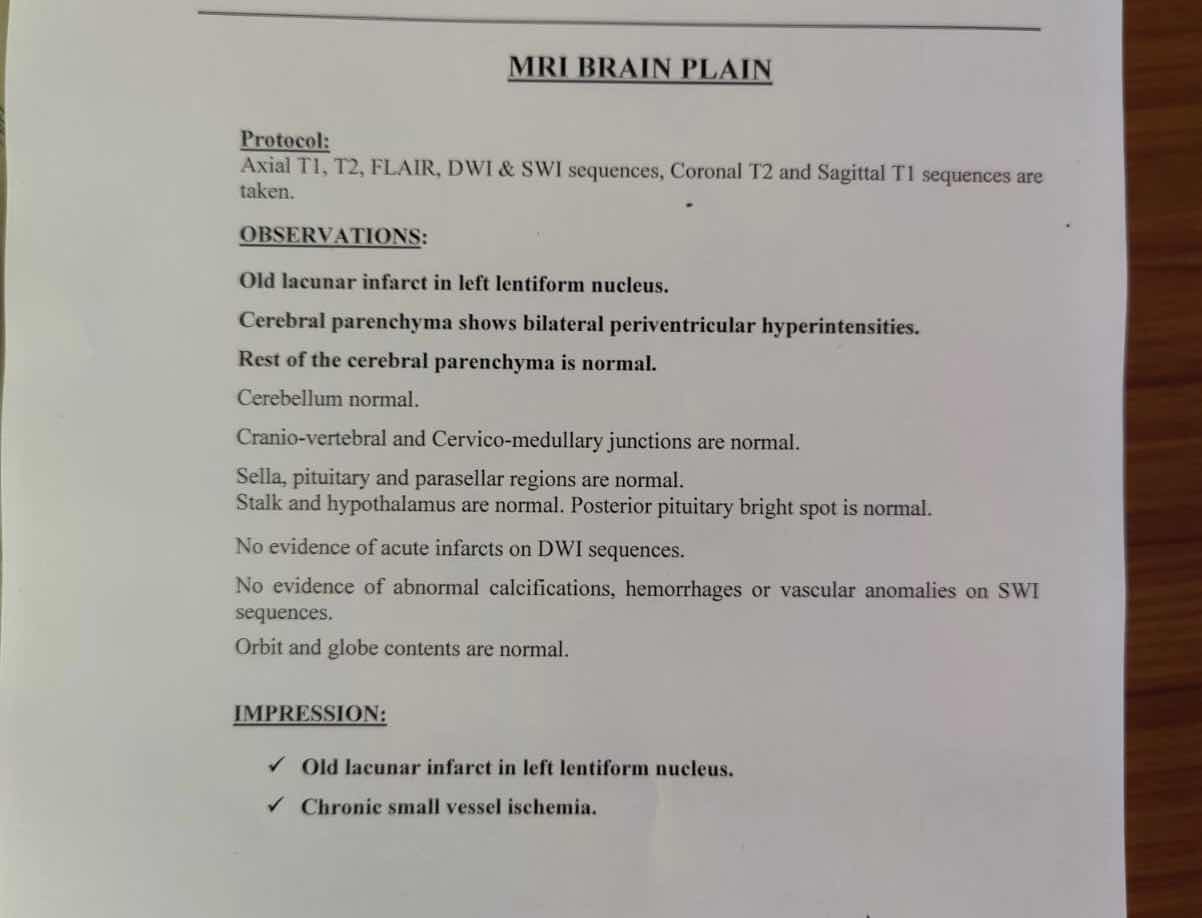
MRI DONE:
2D ECHO :

ECG: shows sinus rhythm with left ventricular hypertrophy. (Lyon Sokolow criteria)

Diagnosis: Myoclonic jerks secondary to PCA STROKE
23/2/22
S: Decreased responsiveness, Involuntary movements of head and hands
O:
Temp: 97.4
BP: 130/70
PR: 80bpm
RR: 17cpm
SpO2: 98% at RA
CVS: S1 S2 +
RS: BAE +
CNS: E4V5M6, B/L pupils NSRL
P/A: soft, non tender
A:
Myoclonus jerks secondary to PCA stroke
P:
1. Inj. PAN 40mg IV/OD
2. Inj. THIAMINE 2amp in 100ml NS/IV/TID
3. Inj. LEVIPILL 500mg IV/BD
4. Inj. MONOCEF 1gm/IV/BD
5. IVF NS& RL
6. BP,PR and temperature 4th hourly monitoring
24/2/22
ICU bed 5
S: Decreased responsiveness, Involuntary movements of head and hands
O:
Temp: 98.2
BP: 120/70
PR: 73bpm
RR: 17cpm
SpO2: 96%at RA
CVS: S1 S2 +
RS: BAE +
CNS: E4V5M6, B/L pupils NSRL
P/A: soft, non tender
A:
Myoclonus jerks secondary to PCA stroke
P:
1. Inj. PAN 40mg IV/OD
2. Inj. THIAMINE 2amp in 100ml NS/IV/TID
3. Inj. LEVIPILL 500mg IV/BD
4. Inj. MONOCEF 1gm/IV/BD
5. IVF NS& RL
6. BP,PR and temperature 4th hourly monitoring
MRI done yesterday night, provisional report impression: chronic small vessel ischemic changes seen.
Investigations (24/2/22)
- I/V/O Anemia the following investigations were sent:
- Serum ferritin: 113.4
- Retic count: 1.3%
- Corrected Reticulocyte count: 0.798 calculated using formula Retic count* Pt HCT/Normal HCT. Impression: hypoproliferative marrow.
- Peripheral smear: Normocytic Normochromic RBCs with few microcytes. WBCs increased on smear and platelets adequate.

Low Retic count here could point towards anemia of chronic disease or renal failure, in this context.

- I/V/O Hyponatremia(Na=128mEq/L)
- Serum electrolytes: Na-137, K-3.8, Cl-103
- Urine electrolytes: Na-150, K-14.3
- Urine urea: 409
- Serum osmolality: 269 (calculated using formula 2*Na+Blood glucose/18+BUN/1.8)
- Urine osmolality: 476 calculated using 2(Urinary Na + K)+Urinary urea/2.8+urinary glucose/18
Impression: Hypoosmolar Hyponatremia
- Thyroid profile: T3: 0.39, T4: 7.34, TSH: 3.33
- HbA1c: 6.7
LFT:
Tb: 0.54
Db: 0.20
AST: 54
ALT:33
AlkP:126
TP:5.3
Alb: 3.4
A/G: 1.83
Gait:
25/2/22
S: Right knee joint pain since yesterday night.
burning micturition +
NO fever spikes
O:
Temp: 98.2 f
BP: 160/90 mm hg
PR: 88bpm
RR: 18cpm
SpO2: 99%at RA
CVS: S1 S2 +
RS: BAE +
CNS: E4V5M6, B/L pupils NSRL
P/A: soft, non tender
Local examination : Right knee joint - mild swelling, with local rise of temperature + tenderness +
No erythema
- Thrombophelitis + at right forearm cannula site
A:
Myoclonus seizures with h/o of HTN & DM
Cue (24/2/22) i/v/o burning micturition
Pus cells : 3-4
Epithelial cells :2-3
Alb : trace
P:
1. Inj. LEVIPILL 500mg IV/BD
2. TAB. NEUROKIND PO/ OD
3.tab metformin 500mg OD
4. Tab. Clinidipine 10 mg po / OD
5) BP,PR and temperature 4th hourly monitoring
6) Planning for x- ray knee AP, lateral views, after taking ortho opinion

X ray done for Right knee pain(25/2/22)




Comments
Post a Comment